On March 11, 2026, the Supreme Court of India granted permission for the country’s first-ever execution of passive euthanasia India has witnessed. This historic order in Harish Rana v. Union of India marks a watershed moment in constitutional law. For the first time, the Court moved beyond theoretical recognition to actual implementation. Specifically, it implemented the right to die with dignity under Article 21. Consequently, this decision affects how legal practitioners will counsel clients on Advance Medical Directives and Living Wills for years to come.
Introduction: A Landmark Moment for Article 21
The Supreme Court’s order dated March 11, 2026, represents more than just another ruling. It signifies the first practical application of the guidelines laid down in Common Cause v. Union of India (2018). For eight years, the legal framework existed only on paper. However, no patient had actually benefited from the procedure until now.
The Constitutional Significance
Justice J.B. Pardiwala, delivering the main judgment, articulated the profound nature of this decision. He stated that the ruling “does not neatly fit within logic and reason alone.” Rather, “it sits in a space between love, loss, medicine and mercy” according to the SCC Online report.
The Court reaffirmed that the right to live with dignity under Article 21 inherently includes the right to die with dignity. This principle, first recognized in Gian Kaur v. State of Punjab (1996), has now found its fullest expression. Therefore, passive euthanasia India jurisprudence has evolved from abstract right to concrete remedy.
Why This Case Matters Now
Previously, lawyers advising clients on Living Wills operated in uncharted territory. The 2018 judgment created the legal framework but offered no tested procedure. However, this March 2026 order provides the first precedent for how courts actually evaluate such requests.
Moreover, the judgment clarifies several procedural ambiguities that troubled practitioners. For example, the Court addressed whether CANH (Clinically Assisted Nutrition and Hydration) constitutes medical treatment. Additionally, it established the “best interests” framework for evaluating withdrawal requests.
Case Summary: The March 11, 2026 Order
The petitioner, Harish Rana, was 32 years old when the Supreme Court delivered this order. He had been in a Persistent Vegetative State (PVS) for 13 years following a tragic accident. Specifically, while pursuing his B.Tech at Punjab University at age 20, he fell from the fourth floor of his paying guest accommodation.
Medical Condition and Treatment History
The fall caused diffuse axonal injury, a severe form of brain damage. Harish required ventilating support, tracheostomy, and sustained treatment initially. Subsequently, his feeding transitioned from a nasogastric tube to a surgically placed PEG tube. This tube required hospital replacement every two months.
Throughout these 13 years, Harish showed no evidence of awareness of his environment. He remained incapable of interaction, completely bedridden, and suffered painful bedsores. Furthermore, this occurred despite his mother’s attentive nursing care. The LiveLaw report details these medical findings comprehensively.
Procedural Journey Through Courts

The legal battle spanned multiple courts and two years. First, Delhi High Court dismissed the petition in July 2024. It observed that the petitioner was not terminally ill. Subsequently, the Supreme Court initially refused to entertain the plea in August 2024. However, it directed Uttar Pradesh to bear treatment expenses.
In 2025, the Supreme Court directed the constitution of Primary and Secondary Medical Boards. Both Boards unanimously recommended withdrawal of CANH. Consequently, this unanimity proved crucial to the final outcome.
Key Legal Issues Decided
The Court addressed two fundamental questions. First, whether CANH constitutes medical treatment or basic sustenance. Second, what standard should guide decisions when the patient cannot consent.
On the first issue, the Court held that CANH is medical treatment. Specifically, it represents a “technologically mediated intervention,” not basic care. This classification matters significantly. In short, medical treatment can be withdrawn; basic sustenance cannot.
On the second issue, the Court established a “best interests” framework with seven guiding factors. Therefore, the correct question becomes: Is it in the patient’s best interests that life be prolonged by continuing treatment?
Tracing the Legislative History: From Aruna Shanbaug to 2018
Understanding passive euthanasia India jurisprudence requires examining its evolution through landmark cases. The journey spans three decades and multiple judicial iterations.
The Aruna Shanbaug Case (2011)
The case of Aruna Ramchandra Shanbaug v. Union of India first brought euthanasia into Indian legal discourse. Aruna Shanbaug, a staff nurse at KEM Hospital Mumbai, suffered devastating injuries in November 1973. A sweeper sodomized her and twisted a dog chain around her neck. As a result, she suffered brain damage from oxygen deprivation.
She remained in PVS for 36 years when Pinki Virani petitioned the Court. Justice Markandey Katju, writing for the Bench, acknowledged the complexity. He stated: “Euthanasia is one of the most perplexing issues which the courts and legislatures all over the world are facing today.”
The petition was ultimately dismissed. KEM Hospital staff, considered the true next friends, opposed withdrawal. However, the Court laid down initial guidelines for passive euthanasia. Specifically, it required High Court approval and a committee of three doctors to examine the patient.
Common Cause v. Union of India (2018)
A five-judge Constitution Bench delivered this transformative judgment. Chief Justice Dipak Misra led the Bench, which recognized the right to die with dignity as a fundamental right under Article 21. The full judgment established crucial distinctions.

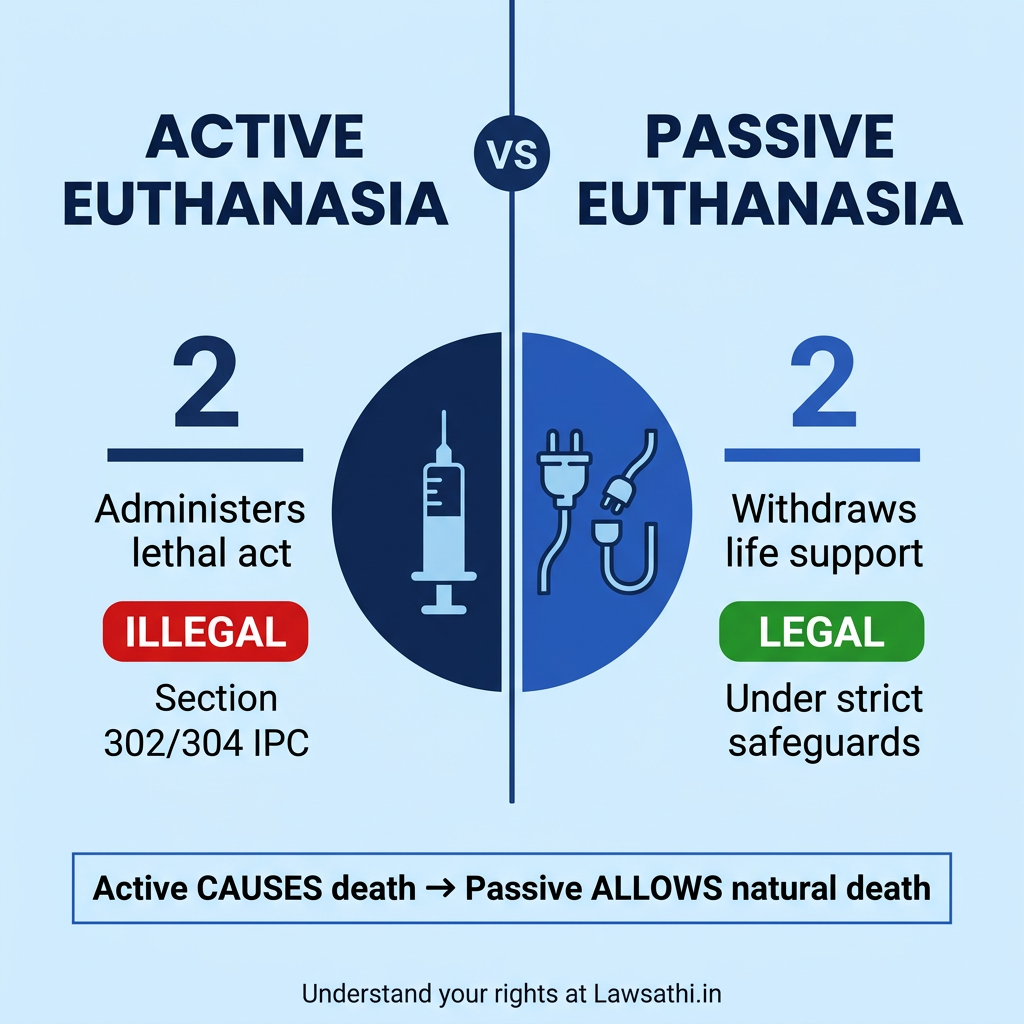
Active euthanasia entails positive affirmative acts, such as administering lethal drugs. This remains illegal under Section 302 or 304 IPC. In contrast, passive euthanasia involves withdrawal or withholding of life support, allowing natural death. This became legally permissible.
The judgment also recognized Advance Medical Directives (AMD), commonly called Living Wills. Therefore, an adult with mental capacity can refuse medical treatment, including life-saving devices, through an AMD.
The 2023 Simplification Amendment
The original 2018 guidelines proved too cumbersome for practical use. In fact, no case was processed under them for five years. In January 2023, the Supreme Court simplified the procedure substantially.
Key changes included removing JMFC countersignature requirements. As a result, two witnesses plus a notary or gazetted officer became sufficient for authentication. Additionally, the Medical Board decision timeline shortened to 48 hours. Furthermore, doctor experience requirements reduced from 20 years to 5 years. According to the SCC Online analysis, these changes finally made the framework workable.
Procedural Compliance: A Guide for Legal Practitioners
For lawyers advising clients on Living Will India matters, understanding current procedural requirements is essential. The March 2026 order and 2023 amendments have substantially streamlined compliance.
Drafting Valid Advance Medical Directives
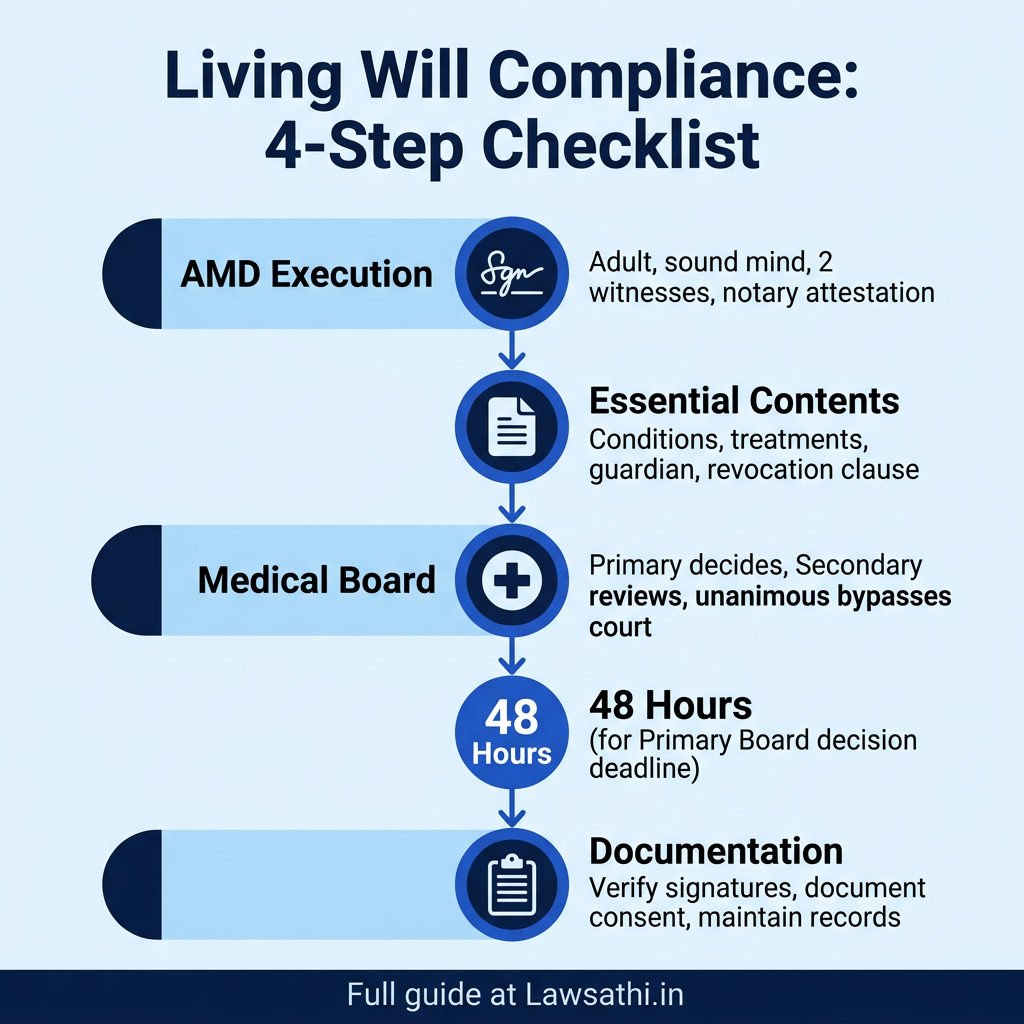
An AMD must meet specific execution requirements to be valid. First, the person executing it must be an adult of sound mind. They must execute it voluntarily, without coercion or inducement. Additionally, full knowledge and comprehension of consequences is mandatory.
Essential contents include: – Clear statement of when treatment may be withdrawn – Specific treatments to be withheld – Name of authorized guardian or close relative – Statement confirming understanding of consequences – Revocation clause
Authentication requirements (post-2023) require signature before two independent witnesses. Furthermore, a notary or gazetted officer must attest the document. Consequently, JMFC countersignature is no longer mandatory, simplifying execution considerably.
Medical Board Constitution and Procedure
When a patient in PVS or terminal condition is admitted, hospitals must constitute a Primary Medical Board. Doctors need minimum 5 years of experience. Additionally, subject experts of the relevant specialty must be included. The Board must decide within 48 hours of case referral.
The Secondary Medical Board reviews the Primary Board’s decision. Specifically, at least one doctor must be nominated by the Chief Medical Officer. If both Boards agree unanimously, court intervention becomes unnecessary. Therefore, this procedural efficiency explains why Harish Rana’s case proceeded smoothly.
Documentation Best Practices for Lawyers
When advising clients, verify proper AMD execution meticulously. First, check witness signatures and notary attestation carefully. Second, ensure the document clearly specifies triggering conditions. Finally, confirm the named guardian is willing and available.
During implementation, document consent of next of kin in writing. Additionally, maintain records of Medical Board proceedings thoroughly. Furthermore, prepare for potential High Court approach if Boards disagree. The Legal Journey of Living Wills provides comprehensive guidance on these requirements.
Ethical and Legal Dilemmas for Law Firms
Passive euthanasia India practice raises complex ethical questions. Therefore, lawyers must navigate these sensitively while protecting client interests.
The Active Versus Passive Distinction
The law draws a bright line between active and passive euthanasia. Active euthanasia involves affirmative acts causing death. In contrast, passive euthanasia permits natural death by withdrawing intervention.
For clients confused about this distinction, explain through examples. Administering a lethal injection constitutes active euthanasia. However, removing a ventilator that sustains artificial breathing represents passive euthanasia. In short, the former is murder; the latter is legal under safeguards.
Potential for Misuse and Safeguards
Critics argue that passive euthanasia creates a “slippery slope.” For example, relatives might seek withdrawal for property inheritance. Additionally, vulnerable patients may face coercion to execute AMDs. Furthermore, the elderly could feel pressured to not burden families.
The legal framework includes multiple safeguards against such abuse. First, Medical Board oversight provides independent medical assessment. Second, family consent requirements ensure collective decision-making. Finally, judicial review remains available when disputes arise.
Liability Protection for Medical Practitioners
Doctors following Common Cause guidelines receive legal protection. However, deviation from procedure exposes them to prosecution under Section 304 IPC. Therefore, the key is documenting every step meticulously.
Lawyers counseling hospitals should advise: – Maintain detailed records of Board proceedings – Obtain informed consent from family in writing – Follow the “best interests” assessment framework – Ensure palliative care accompanies any withdrawal
The LiveLaw analysis examines these liability aspects comprehensively.
Counseling Clients Through Difficult Decisions
Families facing these situations need compassionate legal guidance. They often struggle with guilt and uncertainty. Therefore, lawyers should explain that passive euthanasia is not about choosing death. Rather, it is about not artificially prolonging suffering.
Justice Viswanathan’s words in the March 2026 order offer perspective. He stated: “His family never left his side… to love someone is to care for them even in the darkest times.”
Conclusion: The Future of Right to Die in India
The March 2026 order transforms passive euthanasia India jurisprudence from theory to practice. After eight years of dormancy, the Common Cause framework finally demonstrated its workability. Consequently, this precedent will guide future applications and judicial approaches.
Strengthening Bodily Autonomy
This judgment strengthens individual autonomy over one’s body substantially. Specifically, the Court confirmed that Medical Boards can make final decisions when unanimous. Therefore, judicial intervention is not always necessary. This efficiency benefits families facing prolonged suffering.
Moreover, the classification of CANH as medical treatment is significant. It clarifies that artificially administered nutrition can be withdrawn. As a result, this expands the scope of what constitutes permissible withdrawal.
The Need for Parliamentary Legislation
Judicial guidelines, however well-crafted, remain interim measures. The Supreme Court explicitly recommended that Parliament enact comprehensive legislation. Therefore, the Union Government should address this through subject-specific statutes.
Law Commission’s 241st Report (August 2012) already provided recommendations. The Medical Treatment of Terminally Ill Patients Bill was proposed but never enacted. However, legislative action would provide greater certainty and uniformity nationwide.
Practical Takeaways for Legal Professionals
For practitioners handling such cases: 1. Verify AMD execution meets current simplified standards 2. Ensure Medical Boards comply with experience and timeline requirements 3. Document family consent and best interests assessment thoroughly 4. Know that unanimous Board decisions bypass court requirements 5. Understand the 30-day reconsideration period can be waived in appropriate cases
The Harish Rana case proves the system works when properly followed. His family’s 13-year struggle ended with dignity because they navigated the procedure correctly.
Stay ahead of critical legal developments. Use LawSathi to track case law updates, manage your medical law clients, and automate your legal research effortlessly.